19 April 2024: Clinical Research
Role of Critical Shoulder Angle in Degenerative Type Rotator Cuff Tears: A Turkish Cohort Study
Mehmed Nuri Tütüncü1ACE*, Yiğit Kültür2BD, Mahmut Kürşat Özşahin3BCD, Nuri Aydın3ABEDOI: 10.12659/MSM.943703
Med Sci Monit 2024; 30:e943703






Abstract
BACKGROUND: This retrospective study investigated the association between the critical shoulder angle (CSA) and the development of full-thickness rotator cuff tears (FTRCTs) in the Turkish population. The CSA is an imaging parameter that quantifies the relationship between the inclination of the glenoid and the lateral extension of the acromion in the coronal plane. The CSA is an anatomical measurement, and higher CSA values have been associated with an increased incidence of FTRCTs. However, there is a lack of data on CSA regarding the Turkish population.
MATERIAL AND METHODS: In this study, CSA measurements were recorded in 2 groups: 50 patients with FTRCT who had arthroscopic repair (group 1) and 50 age- and sex-matched individuals with no FTRCT detected by magnetic resonance imaging (group 2). Sex, age, affected side, dominant side, and smoking status were recorded for each patient. The CSA measurements of the affected sides were performed on true anterior-posterior view radiographs.
RESULTS: The results showed a statistically significant difference between the mean CSA values of group 1 (37.48°) and group 2 (33.53°), P<0.001. CSA values of 36 and above had a sensitivity of 73.58%, specificity of 74.47%, positive predictive value of 75%, and negative predictive value of 74.47% for detecting FTRCT.
CONCLUSIONS: CSA measurement on radiographs is a useful diagnostic tool in the Turkish population, and an above-average CSA value is associated with a significantly increased incidence of degenerative-type FTRCT.
Keywords: Rotator Cuff Tear Arthropathy, Shoulder Joint, shoulder pain, Scapula
Introduction
Full thickness rotator cuff tears (FTRCTs) are among the most common shoulder pathologies, with a reported frequency of 7% to 40% [1]. Determining the exact underlying etiology of an FTRCT is quite challenging, as it is multifactorial in nature. While age and trauma have been suggested as the most common causes, there is still debate surrounding this topic [2].
Etiological factors that induce rupture are divided into 2 groups: intrinsic and extrinsic. Intrinsic factors include hypovascularity within the tendon, degeneration due to aging, and inflammation, while extrinsic factors affect the tendon from outside, such as bony or soft tissue surrounding the tendon, impingement syndromes, and differences in scapular morphology [2].
Differences in scapular morphology have been extensively studied to better understand FTRCT etiology. Various concepts, such as acromion type, acromion slope, and acromial index, have been introduced [3–5]. Moreover, the vertical slope of the glenoid has been reported to be associated with the formation of rotator cuff tears [5].
In 2013, Moor et al [6] studied the acromial index and glenoid slope in 298 cases and defined the critical shoulder angle (CSA) as the strongest radiological parameter in predicting rotator cuff tears. In their article, the measurement of the CSA is reported as follows. A line connecting the most lateral points of the superior and inferior borders of the glenoid is drawn. Then, a second line extending from the inferior glenoid to the most lateral point of the acromion is drawn. The angle formed between the 2 lines is defined as the CSA. It has been stated that above-average CSA measurements are associated with degenerative-type rotator cuff tears.
Shinagawa et al [7] investigated the Japanese population and reported that the CSA was higher in patients with FTRCTs and lower in patients with primary shoulder osteoarthritis, compared with CSA values in healthy individuals. Gerber et al [8] conducted a biomechanical study and found that in shoulders with a high CSA, compressive forces should be augmented to meet the increased deltoid shear force during abduction and to preserve joint stabilization. Therefore, the force required for the supraspinatus to compensate for the shear forces increases, leading to degeneration and, eventually, tears.
Previous research has shown that individuals with higher CSA values had a significantly increased prevalence of FTRCTs than the normal population [6]. However, the average CSA values for healthy individuals and patients with rotator cuff tears can differ according to racial/ethnic groups [1,6,7]. Therefore, this study aims to investigate the role of CSA – an anatomical variance that can be measured radiologically – in the development of FTRCTs at average and high angles. The study compares measurements in groups with and without FTRCTs in the Turkish population. The results can serve as baseline values for future studies involving the Turkish population.
Material and Methods
PATIENT SELECTION:
Following the approval of the local ethics committee (05/02/2019-A58) in accordance with international agreements (Helsinki Declaration), 100 patients were included in the study: 50 patients who presented to the outpatient clinic with shoulder pain and underwent arthroscopic repair after being both clinically and radiologically diagnosed with FTRCT and 50 age- and sex-matched controls who presented to the outpatient clinic with shoulder pain but did not have FTRCT detected by magnetic resonance imaging (MRI). Informed consent was obtained from each patient.
Each patient case was assessed retrospectively based on the available radiological data and discharge report. Patients who were ≥45 years old, had true shoulder anterior-posterior (AP) view X-rays in compliance with specific criteria, and had arthroscopic repair due to FTRCT were included. Age-matched patients who presented to the outpatient clinic with shoulder pain but did not have a clinical or radiological (MRI) FTRCT diagnosis with available true shoulder AP-view X-rays were recruited as controls.
Exclusion criteria were as follows: history of major trauma, previous shoulder surgery, incompatible true shoulder AP-view X-rays, history of previous glenoid or acromion fractures, severe deformities, avascular necrosis, and infectious or inflammatory arthritis.
Patients who participated in the study were all operated on by the same surgeon (NA), who had 15 years of experience in shoulder surgery. Demographic data regarding sex, age, upper extremity dominance, and smoking status were recorded.
RADIOLOGICAL ASSESSMENT:
A Toshiba Rotanode X-ray tube was used to obtain radiographs; a Philips Ingenia 1.5T MRI system was used for MRI examination. The radiological data of each participant were evaluated by the authors.
Two CSA measurements were performed by 2 different orthopedic surgeons (NA, MNT) for each patient, and the average value was recorded. Preoperative radiographs of the surgical group were taken into consideration. Techniques regarding CSA measurement and true shoulder AP-view X-rays were determined based on criteria established by Moor et al [6].
Theoretically, if the rotation of the scapula changes during imaging, the CSA value can also change. In the present study, radiographs with visible joint space and minimal overlap of the superior and inferior edges of the glenoid were included. In their study, Moor et al [6] reported that flexion/extension or internal/external rotations of up to 20° created a CSA change of a maximum of 2°. They also stated that during scapular rotations above the abovementioned degrees, the measurement could not be made accurately, because the superior and inferior edges of the glenoid were not clear. Therefore, radiographs that were not within the recommended values were not included in our study. If a participant had multiple radiographs, the radiograph with minimal overlap of the superior and inferior glenoid edge was preferred (Figure 1).
STATISTICAL ANALYSIS:
The Number Cruncher Statistical System 2007 (Kaysville, Utah, USA) program was used for statistical analysis. Descriptive statistical methods (mean, standard deviation, frequency, percentage, minimum, maximum) were used to evaluate the data. The intrarater and interrater reliability of CSA measurements were assessed with intraclass correlation (ICC). The Shapiro-Wilk test and graphical models were used to test the normality of quantitative data. For quantitative variables that showed a normal distribution, an independent sample
Power analysis performed based on previous studies in the literature determined that the minimum sample size for each group should be 43, calculated with a power of 80%. Therefore, the sample size for each group was set as 50 (α=0.05, β=0.9)
Results
The study involved 100 patients, with ages ranging from 45 to 74, and a mean age of 58.44±7.43 years; 43% (n=43) of patients were women and 57% (n=57) were men. In group 1, the mean age was 58.54±7.37, while in group 2, it was 58.34±7.57. In group 1, 44% (n=22) of patients were women and 56% (n=28) were men. In group 2, 42% (n=21) of patients were women and 58% (n=29) were men.
In both groups, the right extremity involvement rate was higher than the left, with a total right extremity involvement rate of 57% (n=57) and a left extremity involvement rate of 43% (n=43). In group 1 62% (n=31) of patients smoked, while 38% (n=19) did not. In group 2, 66% (n=33) of patients smoked, while 34% (n=17) did not.
The CSA values of the patients ranged between 27.7° and 42.2°, with a mean value of 35.51°±3.42°. The mean CSA value in group 1 was 37.48°±2.47°, while in group 2, it was 33.53°±3.10°. Excellent intraobserver and interobserver reliabilities were obtained, with an ICC for intrarater reliability of 0.95 (95% CI: 0.92–0.97) and ICC for interrater reliability of 0.94 (95% CI: 0.91–0.96).
There was no statistically significant difference between the 2 groups in terms of age, sex, affected side, upper extremity dominance, and smoking status
A cutoff point for CSA was calculated, and patients with CSA values of 36 and above had a sensitivity of 73.58%, specificity of 74.47%, positive predictive value of 75%, and negative predictive value of 74.47% for detecting FTRCTs (Table 2). The area under the ROC curve was 77.4%, with a standard error of 4.6 (Figure 2). There was no statistically significant relationship between age, sex, dominant extremity, smoking status, affected side, and CSA values of the patients
Discussion
According to our data, there was a statistically significant difference between the group with FTRCTs (group 1) and group without FTRCTs (group 2) in terms of CSA values (
The study group was compared with the age- and sex-matched controls, and age and sex were not significant in terms of FTRCT development. However, it is well established that age is one of the most important risk factors for the development of degenerative FTRCT [6–8]. Several studies have found that rotator cuff tears are more common among men, while others have argued that female sex is also a potential risk factor [10,11]. Abate et al [12], for example, observed that postmenopausal women have an increased risk of developing rotator cuff tears.
In the present study, there was no statistically significant difference between the groups regarding the dominant side. The ratio of the dominant side being the affected side was higher in the study group than in the control group; however, the difference was not statistically significant. While some studies reported a higher incidence of rotator cuff tears on the dominant upper extremity, others have reported the opposite; a consensus has not been reached on this issue [13–15].
Although the rate of smoking was higher in the control group, the difference between the 2 groups was not statistically significant. Numerous studies have demonstrated that the amount and duration of smoking increase the risk of rotator cuff tear development. Baumgarten et al [16] investigated 586 patients with unilateral shoulder pain, 375 of whom were diagnosed with rotator cuff tears. It was also demonstrated that 61.9% of the individuals diagnosed with rotator cuff tears smoked, with an average use of 30.1 packs/year. Consistent with the literature, 64% of the patients who participated in our study smoked. Bishop et al [17] demonstrated an increased incidence of rotator cuff tear development, larger tears, and a higher number of surgical interventions in individuals who smoked. Carbone et al [18] reported that the prevalence of type II tears (34.8%) was higher than that of type I tears (23.2%) in smokers. This finding promotes the notion that smoking could lead to tendon hypovascularity.
Different CSA values have been reported in the literature due to possible anatomical differences between diverse societies and ethnicities. Our goal was to determine the mean CSA value in Turkish society and to assess its role in FTRCT development. This study is one of few Turkish studies investigating the relationship between bone morphology and FTRCT development. The findings will provide baseline values for future studies regarding CSA values involving the Turkish population. The mean CSA value was 33.53° in the group without FTRCTs and 37.48° in the group with FTRCTs. In a similar study conducted in East Asia, the mean CSA value was reported as 32.3° in the group without FTRCTs and 33.9° in the group with FTRCTs [7]. In another study, performed in Japan, the mean CSA value was 33.7° in the group without FTRCTs and 36.3° in the group with FTRCTs. Moreover, it has been suggested that CSA values are not affected by height and weight [7,9,19]. Furthermore, the mean CSA value was reported as 33.59° in the group without FTRCTs and 39.75° in the group with FTRCTs in a study performed in Brazil [1]. In light of this information, we consider the morphological differences between races to affect CSA values.
There have been many other radiological parameters previously defined in the literature. Balke et al [20] reported that acromial slope, type 3 acromion, high acromial index, CSA, short acromiohumeral distance, and lateral acromial angle were associated with rotator cuff tear development. Moor et al [21], on the other hand, reported that among the acromial index, CSA, and lateral acromial angle, CSA has the strongest predictive value for rotator cuff tear development. Pandey et al [22] studied several factors, such as acromial index, subacromial index, lateral acromial angle, CSA, and presence of subacromial osteophytes, and concluded that above-average CSA values and subacromial osteophyte presence have the strongest predictive value for the development of rotator cuff tears.
In the present study, CSA measurements were performed on the radiographs. Several studies have compared CSA measurements on radiographs, MRI, and computerized tomography scans and have concluded that plain radiography had similar reliability to computed tomography and was more reliable than MRI [23,24].
Bjarnison et al [25] conducted a study with 979 patients and concluded that high CSA values did not significantly increase rotator cuff tear; however, low CSA values were associated with primary glenohumeral osteoarthritis. Chalmers et al [26] also reported that high CSA values were not associated with rotator cuff tear development, initial extent, or progression of tears. Moreover, it was pointed out that CSA values did not change over the 4-year follow-up period. However, the authors stated that only 20% of the radiographs met the Suter-Henninger criteria, emphasizing the practical difficulty of using suitable true AP-view X-rays for CSA measurement.
According to our data, in patients with CSA values of 36 and above, the sensitivity of detecting FTRCTs was 73.58%, specificity was 74.47%, positive predictive value was 75%, and negative predictive value was 74.47%. A meta-analysis encompassing 8 studies concluded that CSA measurement is a useful diagnostic tool and that CSA values of 35° and above increase the incidence of FTRCT development [9]. In this respect, our results seem to be compatible with the previous literature.
Since our study had a retrospective design, one of the limitations is that it was not known whether there were existing rotator cuff tears in the contralateral shoulders of the patients selected for the group without rotator cuff tears. If this information was made available, statistical results could be affected. The second limitation, a lack of standardization for true shoulder AP-view X-ray and lack of specifically trained technicians, could be avoided if the study was performed prospectively. A prospective design would result in an increased number of patients with appropriate radiographs and thus increased statistical power. A prospective design would also allow us question the patient’s occupation and shoulder involvement during work, to investigate these factors as separate variables. One of the study’s constraints is that it involved patients with shoulder pain who were part of the control group, and there was no arthroscopic verification of rotator cuff tears in these patients. Finally, our study with 50 control patients and 50 patients with FTRCT in a single center cannot be generalized to the entire population. Although our sample size is compatible with previous studies, multicenter studies with a higher number of participants should be conducted to obtain better data. However, our results could still be important and beneficial in terms of future studies.
Conclusions
Based on the findings of this study, we support the notion that above-average CSA values can be predictive of full-thickness degenerative-type rotator cuff tears. Moreover, the CSA measurement can be regarded as a practical and useful diagnostic tool that can be successfully used in the Turkish population.
Figures
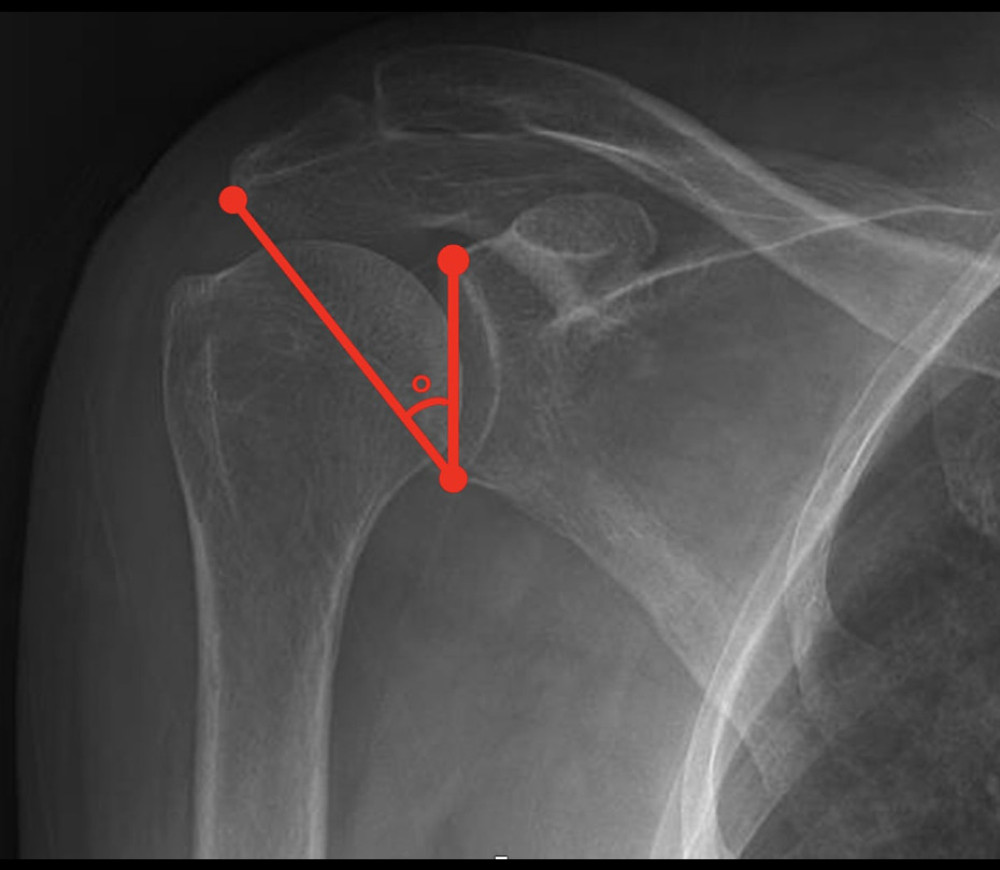 Figure 1. Critical shoulder angle (CSA) measurement technique. A line connecting the most lateral points of the superior and inferior borders of the glenoid is drawn. Then, a second line extending from the inferior glenoid to the most lateral point of the acromion is drawn. The angle formed between the 2 lines is defined as the CSA (Powerpoint, Office for Mac,2023 version: 16.74; Redmond, Washington, USA).
Figure 1. Critical shoulder angle (CSA) measurement technique. A line connecting the most lateral points of the superior and inferior borders of the glenoid is drawn. Then, a second line extending from the inferior glenoid to the most lateral point of the acromion is drawn. The angle formed between the 2 lines is defined as the CSA (Powerpoint, Office for Mac,2023 version: 16.74; Redmond, Washington, USA). 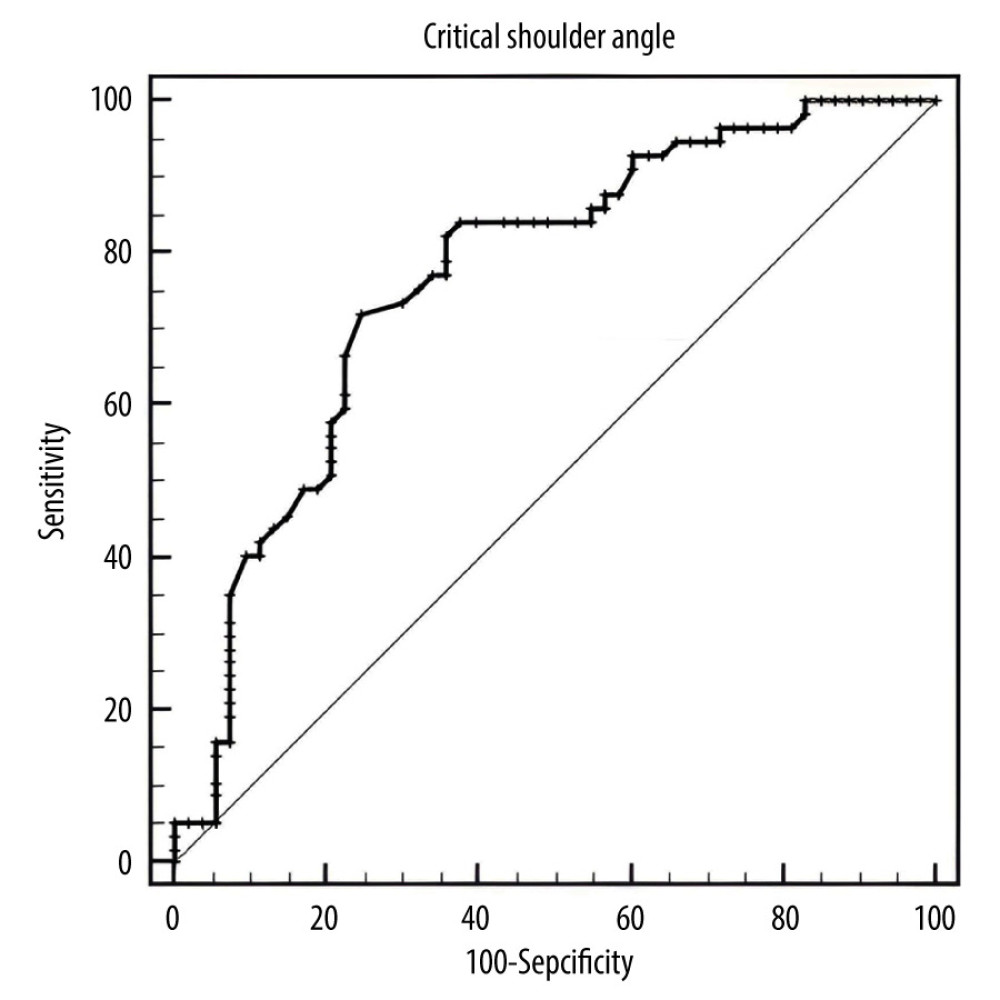 Figure 2. Receiver operating characteristic (ROC) curve for critical shoulder angle (CSA). A cutoff point for CSA was calculated, and patients with CSA values of 36 and above had a sensitivity of 73.58%, specificity of 74.47%, positive predictive value of 75%, and negative predictive value of 74.47% for detecting full thickness rotator cuff tear. The area under the ROC curve was 77.4%, with a standard error of 4.6 (Number Cruncher Statistical System 2007; Kaysville, Utah, USA).
Figure 2. Receiver operating characteristic (ROC) curve for critical shoulder angle (CSA). A cutoff point for CSA was calculated, and patients with CSA values of 36 and above had a sensitivity of 73.58%, specificity of 74.47%, positive predictive value of 75%, and negative predictive value of 74.47% for detecting full thickness rotator cuff tear. The area under the ROC curve was 77.4%, with a standard error of 4.6 (Number Cruncher Statistical System 2007; Kaysville, Utah, USA). References
1. Gomide LC, Carmo TCD, Bergo GHM, Relationship between the critical shoulder angle and the development of rotator cuff lesions: A retrospective epidemiological study: Rev Bras Ortop, 2017; 52(4); 423-27
2. Yadav H, Nho S, Romeo A, MacGillivray JD, Rotator cuff tears: Pathology and repair: Knee Surg Sports Traumatol Arthrosc, 2009; 17(4); 409-21
3. Bigliani LU, Morrison DS, April EW, The morphology of the acromion and rotator cuff impingement: Orthopaedic Transactions, 1986; 10; 228
4. Nyffeler RW, Werner CM, Sukthankar A, Association of a large lateral extension of the acromion with rotator cuff tears: J Bone Joint Surg Am, 2006; 88(4); 800-5
5. Hughes RE, Bryant CR, Hall JM, Glenoid inclination is associated with full-thickness rotator cuff tears: Clin Orthop Relat Res, 2003(407); 86-91
6. Moor BK, Bouaicha S, Rothenfluh DA, Is there an association between the individual anatomy of the scapula and the development of rotator cuff tears or osteoarthritis of the glenohumeral joint?: A radiological study of the critical shoulder angle: Bone Joint J, 2013; 95-B(7); 935-41
7. Shinagawa K, Hatta T, Yamamoto N, Critical shoulder angle in an East Asian population: Correlation to the incidence of rotator cuff tear and glenohumeral osteoarthritis: J Shoulder Elbow Surg, 2018; 27(9); 1602-6
8. Gerber C, Snedeker JG, Baumgartner D, Viehöfer AF, Supraspinatus tendon load during abduction is dependent on the size of the critical shoulder angle: A biomechanical analysis: J Orthop Res, 2014; 32(7); 952-57
9. Song JG, Yun SJ, Song YW, Lee SH, High performance of critical shoulder angle for diagnosing rotator cuff tears on radiographs: Knee Surg Sports Traumatol Arthrosc, 2019; 27(1); 289-98
10. Razmjou H, Lincoln S, Macritchie I, Sex and gender disparity in pathology, disability, referral pattern, and wait time for surgery in workers with shoulder injury: BMC Musculoskelet Disord, 2016; 17(1); 401
11. Pauly S, Stahnke K, Klatte-Schulz F, Do patient age and sex influence tendon cell biology and clinical/radiographic outcomes after rotator cuff repair?: Am J Sports Med, 2015; 43(3); 549-56
12. Abate M, Schiavone C, Di Carlo L, Salini V, Prevalence of and risk factors for asymptomatic rotator cuff tears in postmenopausal women: Menopause, 2014; 21(3); 275-80
13. Milgrom C, Schaffler M, Gilbert S, van Holsbeeck M, Rotator-cuff changes in asymptomatic adults. The effect of age, hand dominance and gender: J Bone Joint Surg Br, 1995; 77(2); 296-98
14. Teunis T, Lubberts B, Reilly BT, Ring D, A systematic review and pooled analysis of the prevalence of rotator cuff disease with increasing age: J Shoulder Elbow Surg, 2014; 23(12); 1913-21
15. Gumina S, Carbone S, Campagna V, The impact of aging on rotator cuff tear size: Musculoskelet Surg, 2013; 97(Suppl 1); 69-72
16. Baumgarten KM, Gerlach D, Galatz LM, Cigarette smoking increases the risk for rotator cuff tears: Clin Orthop Relat Res, 2010; 468(6); 1534-41
17. Bishop JY, Santiago-Torres JE, Rimmke N, Flanigan DC, Smoking predisposes to rotator cuff pathology and shoulder dysfunction: A systematic review: Arthroscopy, 2015; 31(8); 1598-605
18. Carbone S, Gumina S, Arceri V, The impact of preoperative smoking habit on rotator cuff tear: Cigarette smoking influences rotator cuff tear sizes: J Shoulder Elbow Surg, 2012; 21(1); 56-60
19. Watanabe A, Ono Q, Nishigami T, Association between the critical shoulder angle and rotator cuff tears in Japan: Acta Med Okayama, 2018; 72(6); 547-51
20. Balke M, Liem D, Greshake O, Differences in acromial morphology of shoulders in patients with degenerative and traumatic supraspinatus tendon tears: Knee Surg Sports Traumatol Arthrosc, 2016; 24(7); 2200-5
21. Moor BK, Wieser K, Slankamenac K, Relationship of individual scapular anatomy and degenerative rotator cuff tears: J Shoulder Elbow Surg, 2014; 23(4); 536-41
22. Pandey V, Vijayan D, Tapashetti S, Does scapular morphology affect the integrity of the rotator cuff?: J Shoulder Elbow Surg, 2016; 25(3); 413-21
23. Bouaicha S, Ehrmann C, Slankamenac K, Comparison of the critical shoulder angle in radiographs and computed tomography: Skeletal Radiol, 2014; 43(8); 1053-56
24. Spiegl UJ, Horan MP, Smith SW, The critical shoulder angle is associated with rotator cuff tears and shoulder osteoarthritis and is better assessed with radiographs over MRI: Knee Surg Sports Traumatol Arthrosc, 2016; 24(7); 2244-51
25. Bjarnison AO, Sørensen TJ, Kallemose T, Barfod KW, The critical shoulder angle is associated with osteoarthritis in the shoulder but not rotator cuff tears: A retrospective case-control study: J Shoulder Elbow Surg, 2017; 26(12); 2097-102
26. Chalmers PN, Salazar D, Steger-May K, Does the critical shoulder angle correlate with rotator cuff tear progression?: Clin Orthop Relat Res, 2017; 475(6); 1608-17
Figures
Figure 1. Critical shoulder angle (CSA) measurement technique. A line connecting the most lateral points of the superior and inferior borders of the glenoid is drawn. Then, a second line extending from the inferior glenoid to the most lateral point of the acromion is drawn. The angle formed between the 2 lines is defined as the CSA (Powerpoint, Office for Mac,2023 version: 16.74; Redmond, Washington, USA).Figure 2. Receiver operating characteristic (ROC) curve for critical shoulder angle (CSA). A cutoff point for CSA was calculated, and patients with CSA values of 36 and above had a sensitivity of 73.58%, specificity of 74.47%, positive predictive value of 75%, and negative predictive value of 74.47% for detecting full thickness rotator cuff tear. The area under the ROC curve was 77.4%, with a standard error of 4.6 (Number Cruncher Statistical System 2007; Kaysville, Utah, USA). Tables
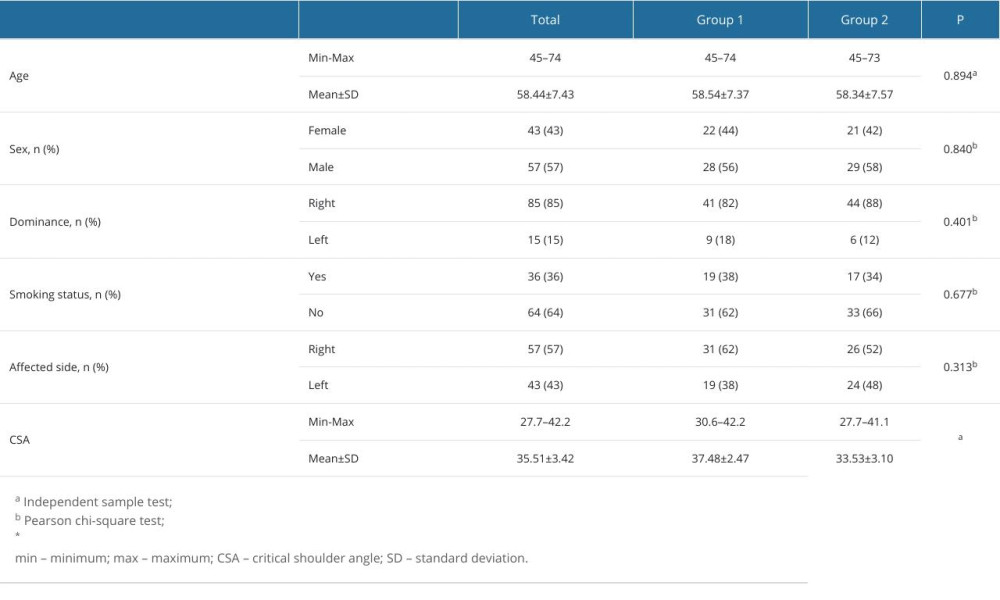 Table 1. Distribution of descriptive properties.
Table 1. Distribution of descriptive properties.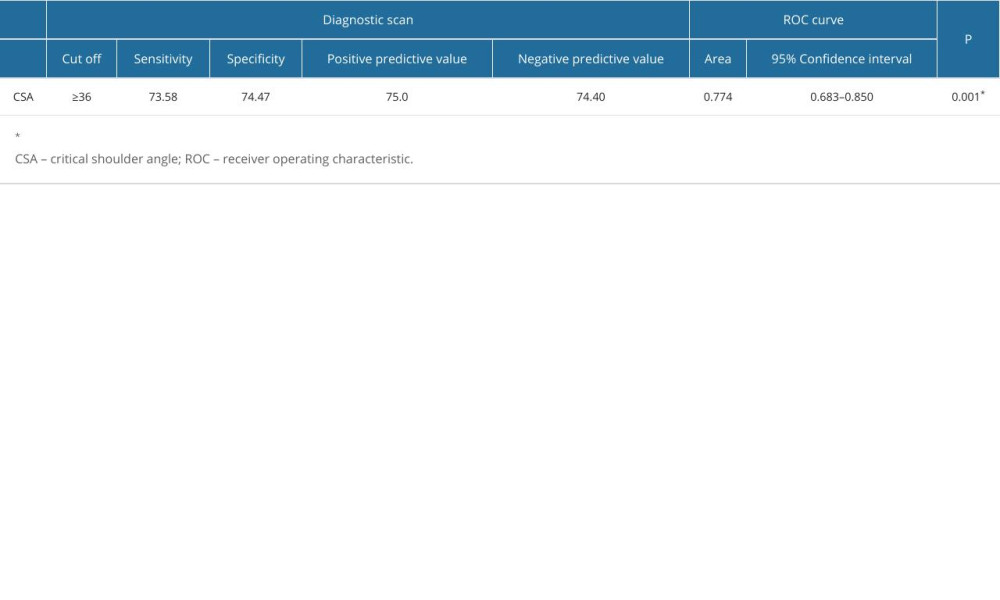 Table 2. Diagnostic screening test results for critical shoulder angle.
Table 2. Diagnostic screening test results for critical shoulder angle.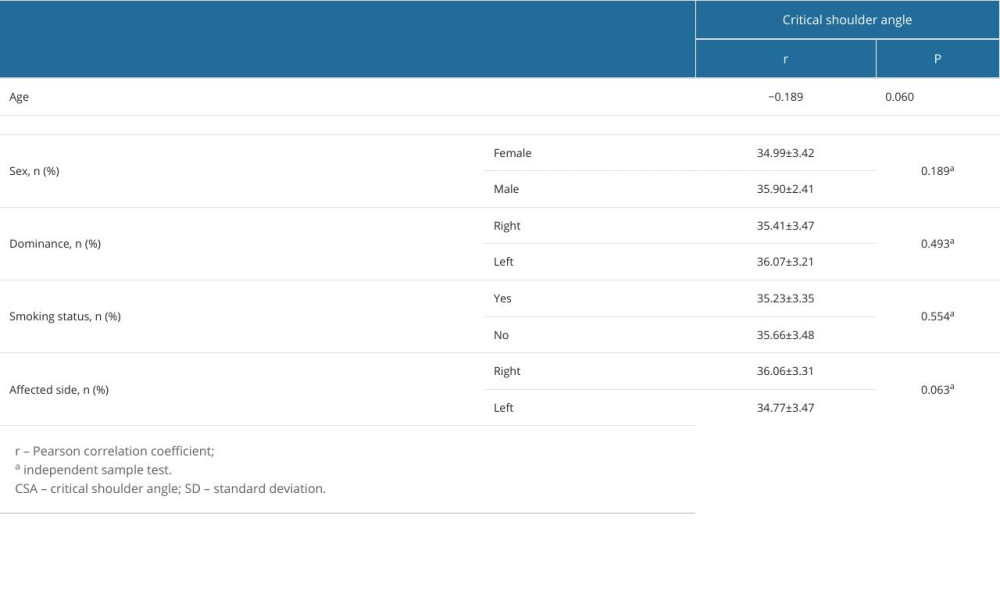 Table 3. Comparison of critical shoulder angle values according to age, sex, dominance, smoking status and affected side.Table 1. Distribution of descriptive properties.Table 2. Diagnostic screening test results for critical shoulder angle.Table 3. Comparison of critical shoulder angle values according to age, sex, dominance, smoking status and affected side.
Table 3. Comparison of critical shoulder angle values according to age, sex, dominance, smoking status and affected side.Table 1. Distribution of descriptive properties.Table 2. Diagnostic screening test results for critical shoulder angle.Table 3. Comparison of critical shoulder angle values according to age, sex, dominance, smoking status and affected side. In Press
08 Mar 2024 : Laboratory Research
Evaluation of Retentive Strength of 50 Endodontically-Treated Single-Rooted Mandibular Second Premolars Res...Med Sci Monit In Press; DOI: 10.12659/MSM.944110
11 Mar 2024 : Clinical Research
Comparison of Effects of Sugammadex and Neostigmine on Postoperative Neuromuscular Blockade Recovery in Pat...Med Sci Monit In Press; DOI: 10.12659/MSM.942773
12 Mar 2024 : Clinical Research
Comparing Neuromuscular Blockade Measurement Between Upper Arm (TOF Cuff®) and Eyelid (TOF Scan®) Using Miv...Med Sci Monit In Press; DOI: 10.12659/MSM.943630
11 Mar 2024 : Clinical Research
Enhancement of Frozen-Thawed Human Sperm Quality with Zinc as a Cryoprotective AdditiveMed Sci Monit In Press; DOI: 10.12659/MSM.942946
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952