03 April 2022: Clinical Research
A Retrospective Study on the Effects of Kinesiology Taping on Edema of the Lower Limb in 14 Patients Following Intramedullary Nailing for Femoral Shaft Fracture
Karen Lanier1ABDEF*, Andrea M. Johnson1ABDEF, Ximena Tapia1ABDEF, Shenae SamuelsDOI: 10.12659/MSM.936619
Med Sci Monit 2022; 28:e936619






Abstract
BACKGROUND: Kinesiology tape indications of use include pain mitigation, neurosensory input, and promotion of circulation. Current evidence suggests that residual functional limitations following intramedullary nailing of the femoral shaft may be due to soft tissue injury and compromise. This retrospective study from a single center aimed to compare the effects of kinesiology taping on edema of the lower limb in 14 patients following intramedullary nailing for femoral shaft fracture.
MATERIAL AND METHODS: The randomized control trial design consisting of 2 groups totaling 14 patients. The intervention group (n=7) received standard therapy and kinesiology tape decompression/fan application. The control group (n=7) received standard therapy with no kinesiology tape. Outcome measures included limb girth tape measurements, Visual Analog Scale (VAS) for pain, involved knee ROM goniometry, and Timed Up and Go (TUG).
RESULTS: Results of this study showed there was a decrease in limb volume in the control group and an increase in limb volume in the intervention group. Both groups had improvements in TUG scores. The only statistically significant finding was among the control group, which had a decrease of 1.6 in mean VAS score before and after IM nailing (P=0.010).
CONCLUSIONS: In this study from a single center, kinesiology tape in patients with intramedullary nailing for femoral shaft fracture did not significantly reduce the volume of the lower limb, reduce pain, or improve postoperative mobility. The only significant improvement from the use of kinesiology tape was improved active knee extension due to improvement in quadriceps force.
Keywords: acute pain, Edema, Femur, Bone Nails, Femoral Fractures, Fracture Fixation, Intramedullary, Humans, Lower Extremity, Range of Motion, Articular
Background
Femoral shaft fractures are commonly seen in multi-trauma patients following high-impact mechanisms, such as motor vehicle accidents, work injuries involving machinery, as well as falls from elevated heights [1]. Treatment of femoral shaft fractures is dependent on multiple factors, including co-morbidities, additional injuries, and the current medical status of the patient [1]. The criterion standard surgical intervention for femoral shaft fractures is intramedullary fracture fixation [1]. Intramedullary (IM) nailing of the femur is a common surgery performed following a fracture of the femoral shaft [2]. Intramedullary nailing of femoral shaft fractures involves a specially designed metal rod which is inserted into the marrow canal of the femur [2]. An IM nail can be inserted into the canal either at the hip or the knee through a small incision [2]. During this operation, the bone fragments are repositioned into their normal alignment and then held together with special screws attached to both ends of the nail. Intramedullary nailing provides strong, stable, full-length fixation [2].
The rod that is inserted into the femur following reduction of the fracture fragments is kept in place by screws placed perpendicularly to the rod at the proximal and distal ends [2]. The distal screw insertion typically leads to significant spread of swelling at the knee joint, affecting knee range of motion (ROM) and kinematics during functional tasks [2]. Although this surgery provides stability to the fragmented femur following a fracture, it also leads to difficulty with improvement in regaining independence for mobility such as getting in and out of a bed or a chair, and walking [2].
Current evidence suggests that residual functional limitations, impairments, and disabilities following IM nailing of the femoral shaft may be due to soft tissue injury and compromise as a result of trauma at the time of injury and/or surgery [2]. The focus of rehabilitation postoperatively is aimed toward improving knee effusion, leg edema, quadriceps control, hip abduction strength, and a normalization of gait [2]. Interventions typically incorporate gait training, ROM activities, physical therapy modalities, stretching, balance and proprioception activities, and conditioning [2]. Knee ROM and edema management are a priority of the postoperative rehabilitation protocol due to their effects on volitional control of the quadriceps, a common residual deficit that can linger up to 8 months after surgery [2]. Edema, muscle guarding (particularly of the quadriceps), and pain all limit the ROM, and consequently, the knee kinematics of the involved lower extremity [2]. This will ultimately result in a slower and limited return to function and preinjury activities.
Kinesiology tape is a modality originally developed in the 1970s to help maintain joints in a less painful position or alignment [3]. This modality has now evolved with research to include indications of uses such as pain mitigation, neurosensory input, and promotion of circulation, or facilitation of lymphatic drainage [3,4]. First, because the skin is the largest sensory organ of the body, with constant feedback to the brain, application of kinesiology tape stimulates mechanoreceptors to block pain receptors [5,6]. Systematic reviews and research on the sensory-motor relationship have supported the effects of kinesiology tape on pain reduction and allowing faster recovery or return to activity due to minimizing nociception-induced motor inhibition [7]. Second, neurosensory input by kinesiology tape is based on the concept of Hilton’s Law, which states that input to the skin also stimulates the tissues beneath it, including muscles and joints, as the same nerve supplies them all [8]. There is research supporting increased activation of the somatosensory cortex when kinesiology tape is applied to the skin [9]. Third, wavelike ridges designed in the tape have been shown through imaging to microscopically lift the skin, forming convolutions to increase interstitial space [10]. This upward lift pulls on the skin, fascia, and periosteum, which in turn dilates capillaries and lymphatic vessels. This decompression results in decreased inflammation and decreased pain [3,10].
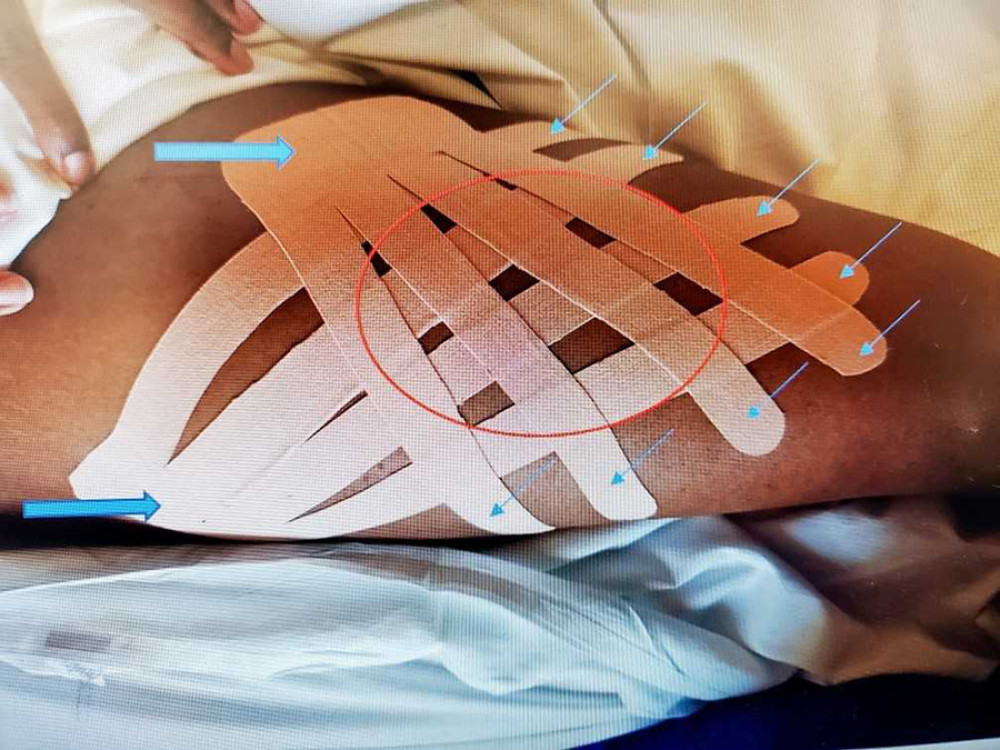
The shape, direction, and tension of application of kinesiology tape has been studied to determine the effects it has on the previously stated indications of use [11]. With decompression, it is suggested that the tape be applied, with minimal to no tension, in a woven pattern across the affected area, using small projected fingers of tape aiming distally toward the area of swelling [11]. Therefore, the anchor of tape located just above the projecting fingers of tape would be placed closest to the proximal lymph nodes in the swollen area (Figure 1). This application is called the fan method [11]. When kinesiology tape is used for indication of edema, the upward pull of the tape created by the ridges embedded in the material creates a pressure gradient between the top layer of skin and underlying tissues [5]. This space thus allows edema to move into the lymphatic vessels and be eliminated from the body [5]. Tsau et al suggested that kinesiology tape could replace the less compliant bandages for stage 1 lymphedema of the upper limb after lymphadenectomy due to breast cancer [4]. However, there is minimal and inconclusive evidence that this kinesiology tape application is effective for decreasing limb volume.
Similar studies on kinesiology taping and the effect of postoperative swelling have been completed for other orthopedic diagnoses, including total knee arthroplasty (TKA) and Ilizarov application, an external fixator for non-union fractures [12]. Bialoszeski et al found that the application of kinesiology taping produced a significantly faster reduction of lower limb edema compared to lymphatic massage alone after performing the Ilizarov method [12]. However, a study looking at postoperative swelling following TKA found that patients did not have a significant improvement in swelling with kinesiology taping compared to treatment with the A-V Impulse System, a sequential compression device that promotes circulation and venous return in the legs [13]. However, kinesiology taping was considered to be equivalent to sequential compression for edema of the limb after TKA [13].
Research on this topic is scarce. No known or published studies have been conducted to determine the effect of kinesiology tape on limb volume after IM nailing of femoral shaft fractures. Therefore, this retrospective study from a single center aimed to compare the effects of kinesiology taping on edema of the lower limb in 14 patients following intramedullary nailing for femoral shaft fracture.
Material and Methods
PARTICIPANTS:
Memorial Healthcare System’s Internal Review Board Chairman, Wayne G. Riskin, M.D., FACP, approved this study on 05/08/2019 and assigned this study project number MHS.2019.025. Informed consent was obtained from all subjects prior to enrollment and initial assessment, as required for protection of human participants. Consent forms included details on the purpose of the study, benefits and risks of participation, voluntary right to participate and withdraw, and confidentiality of records and data sharing. Authorization to release protected health information was also requested as part of the informed consent.
Subjects were recruited from an inpatient rehabilitation setting and met the inclusion/exclusion criteria. Inclusion criteria included subjects 18 years old and older. Included patients were status post intramedullary nailing of femur with no weight-bearing restrictions, as restrictions have an impact on venous return and edema in the restricted extremity. Included patients were also ambulatory since subjects were required to complete the Timed Up and Go (TUG) test, which requires walking with or without an assistive device for a minimum of 20 feet. Exclusion criteria included weight-bearing restrictions, active infection, non-ambulatory status, open wounds of thigh, tape allergy, acute deep vein thrombosis, current cancer diagnosis, decreased or altered sensation, and heart and/or kidney congestion.
DESIGN AND MATERIALS:
This study included an intervention and control group. The intervention group consisted of patients receiving standard therapy care with traditional kinesiology tape fan method application. The tape was applied 3 times per week during the patient’s rehabilitation stay. The control group consisted of patients receiving standard therapy care and no kinesiology tape application. Standard therapy intervention was given to participants for both groups. Standard therapy intervention involved bed mobility training, transfer training, gait training, practice of activities of daily living, therapeutic exercise, and thermal modalities.
The taping was completed by physical therapists or occupational therapists who were trained and completed competencies in the fan application for a total of 3 times per week. For the involved limb, two 4-inch strips of RockTape® (California) kinesiology tape were used and cut into finger projections to create the weave basket shape across the thigh area. The single tip of the strip was placed proximal to the thigh area with the finger projections leading distally toward the area of swelling, or mid-thigh (Figure 1).
PROCEDURES:
Outcome measures included limb girth tape measurements, Visual Analog Scale (VAS) for pain, involved knee ROM goniometry, and the TUG functional outcome measure. Limb girth tape measurements were taken for limb circumference at specific landmarks above the knee joint using a tape measure [14]. There was a consistent starting mark 2 inches below the inguinal fold with measurements taken below the marked line every 4 cm going toward the knee joint. Five measurements was taken from proximal to distal direction for both the involved limb and the uninvolved limb for comparison as a control measure.
The VAS is a subjective measure in which patient rate their pain at rest and during activity from 0 to 10, with zero equivalent to no pain and 10 denoting the worst pain they have ever experienced [15]. For this study, pain during activity was measured following the TUG outcome measure.
Knee ROM goniometry included use of a goniometer to determine the degrees of flexion occurring at the knee joint, which should change proportionately with LE edema [16]. This measurement was conducted with each subject in supine position. Both active and passive knee flexion and extension were measured for the involved limb.
Lastly, the TUG functional outcome measure provides an estimate of fall risk and provides a tracking of change in time needed to complete the functional task of standing up from a sitting in a chair, walking 3 meters, and sitting down in a chair [17]. The patient was asked to stand up from a chair, walk 3 meters to a marker, walk around the marker, and return to the chair to sit down at a comfortable but fast pace [17]. Lower-extremity edema, pain, and knee ROM were hypothesized to have an impact on the patient’s performance of the TUG, leading to an increased time to perform the assessed functional tasks.
Assessment of outcome measures were completed by the research investigators who were blinded to the group in which subjects were randomized. This was accomplished by having treating therapists remove taping prior to re-assessment. The assessment of outcome measures occurred on the third day of admission prior to initial tape application, and the day following the patient’s third and final tape application, considering all 3 tape applications were completed. Collection of data was conducted by a separate recorder who was not involved in the intervention or assessment of the outcome measures. Patients were identified by first and last name initials with medical record number for confidentiality.
STATISTICAL ANALYSIS:
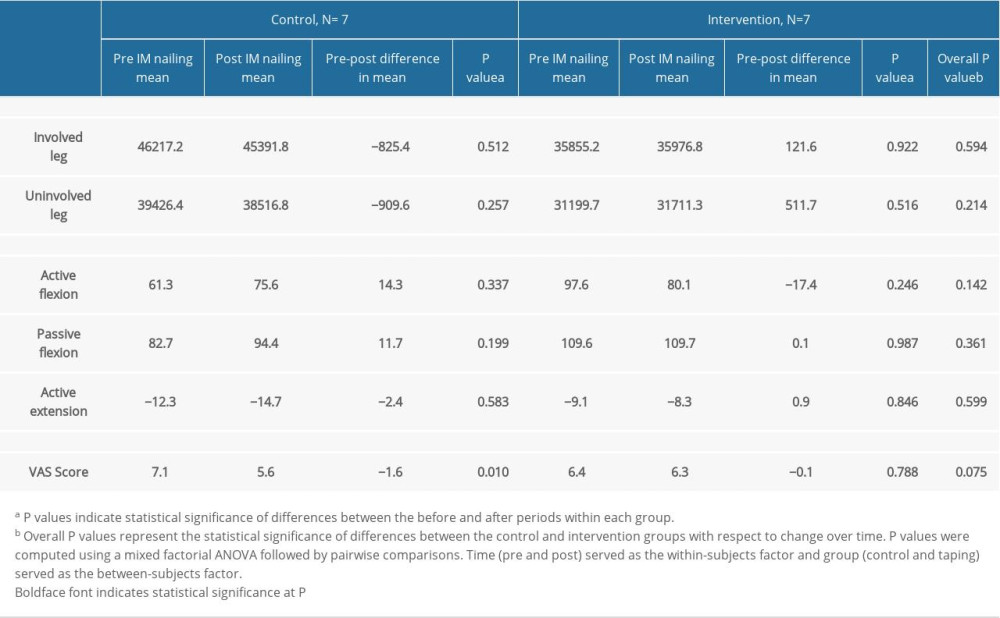
For normally distributed variables, a mixed factorial analysis of variance followed by pairwise comparisons was used to determine the statistical significance of the pre-post differences in mean outcomes within each group, as well as to determine the statistical significance of mean differences between the control and taping groups with respect to change over time. Results are presented in Table 1. Given the non-normality of the variables passive extension and TUG scores, a Wilcoxon signed-rank test was conducted to determine if there were statistically significant changes from before intervention to after intervention within each group. To determine if there were statistically significant differences between the 2 groups during each time period, a Kruskal-Wallis H test was conducted.
Results
OUTCOMES:
There were a total of 14 patients in this study. The only statistically significant finding was in the control group, which had a decrease of 1.6 in mean VAS score, pre-post IM nailing (P=0.010). While the intervention group had increases pre-post in mean total limb volume (involved/uninvolved), active extension, and passive flexion, these differences did not reach statistical significance. The intervention group had decreases in mean active flexion, as well as a very small decrease in VAS score; however, these differences did not reach statistical significance. There were no statistically significance differences in changes over time between the control and intervention group (Table 1).
TIMED UP AND GO SCORES:
Results of the Wilcoxon signed-rank test suggest that in the control group, median TUG score decreased from 122.5 s in the pre period to 45.3 s in the post period. The intervention group also saw a decrease in median TUG score from 85.6 s to 41.8 s. However, these changes in TUG score were not statistically significant in the control group (
The Kruskal-Wallis H test showed that there was no statistically significant difference in TUG scores between the 2 groups (
PASSIVE KNEE EXTENSION:
Results of the Wilcoxon signed-rank test suggest that in the control group, the median passive extension in degrees remained the same from preintervention to postintervention (0°). However, in the intervention group, the median passive extension changed from −3° in the preintervention period to 0° in the postintervention period. However, these changes in median passive extension were not statistically significant (
Discussion
The aim of this study was to describe the outcomes of kinesiology taping on limb volume status after IM nailing of the femur, consequently reducing pain, and improving knee ROM for more functional independence. Results of this study showed there was a decrease in limb volume for the control group. However, in both the involved and uninvolved limb from preintervention to postintervention, these changes did not reach statistical significance. However, there was an increase in limb volume in the intervention group. This finding raises the question of why subjects in the taping group had an increase in limb volume compared to those who had no kinesiology tape applied. One possibility is that the patients in the taping group felt more restricted in movement with tape applied, knowing they had this modality applied for a study. Also, the possibility that other modalities were avoided with the taping group was considered.
In comparison to previous studies looking at the effect of kinesiology tape on edema after orthopedic surgery such as TKA and Ilizarov application, the present study disagreed with the hypothesis that kinesiology taping reduces postoperative edema. However, a prior study looking at edema after Ilizarov application included the intervention of lymphatic massage for edema in addition to kinesiology taping in the treatment group [12]. Additionally, the study observing the effect of kinesiology after TKA found that kinesiology taping was equivalent to but not better than the effect of sequential compression. However, it is unclear what other standard treatment was used in the TKA study that may have had an effect on edema of the limb after TKA; therefore, the effect of kinesiology taping and sequential compression cancel each other out [13]. Significantly, the major difference in this study is that there was an unexpected increase of edema in the involved limb with kinesiology tape application, but this may be due to the avoidance of other modalities in the intervention group.
The only outcome measure with statistically significant changes from pre- to postintervention was the VAS score in the control group, aligning with the results of decreased limb volume seen. Use of other modalities, including ice and heat, in this group may have also contributed to the decrease seen. However, there was a statistically insignificant decrease in pain in the intervention group from pre- to postintervention despite the increase in limb volume. This may be due to the tactile application of the tape blocking nociceptive signals, or it could be explained by use of other pain treatments, including adjustments of pain medication.
In regards to the involved knee ROM, the intervention group had increases in passive flexion and passive extension. These increases were more than likely due to the decrease in muscle guarding of the quadriceps and hamstrings versus the edema, as the edema was greater after the intervention in the taping group. While the control group also had an increase in passive flexion, passive extension remained unchanged from pre- to postintervention. A decrease in active flexion was seen in the intervention group, which raises the question of whether the patients felt more restricted with tape applied to the thigh area, ultimately leading to less bending of the knee. Therefore, along with increased edema in the intervention group, if taping caused a feeling of restriction that limited movement, this would explain the less active flexion in the involved knee joint after the intervention.
On the contrary, there was a slight increase in active extension observed in the taping group from before to after the intervention. It is hypothesized that this can be a result of the facilitation of the quadriceps, as kinesiology taping has been proven to increase peak torque when applied to the quadriceps [18]. There was an increase in active flexion with a decrease in active extension in the control group. The increase in active flexion is congruent with findings of less edema in the control group, as less edema would allow for more active range of the knee joint. However, the cause of a decrease in active extension in the control group warrants further investigation. Certain factors could have contributed to the decreased active extension seen in the control group, such as fatigue at time of postintervention measurements (following other therapies/end of session) as more activities may have been tolerated at the time of postintervention measurements in comparison to preintervention measurements, but interrater error is a more likely causative factor.
Lastly, although the differences did not reach statistical significance, both the control and intervention groups had improvements in TUG scores, showing more efficiency with the functional tasks of standing and sitting from a chair and walking 20 feet. However, no significant difference was seen between the 2 groups before vs after the intervention.
There were considerable limitations to this study. First, the outcome measure of lower- extremity edema using circumferential tape measurements of different segments of the limb has been shown in prior studies to have more standard error and lower test-retest reliability [19]. Additionally, with all the outcome measures conducted in this study, there were often times that the same patient had 2 different pre- and post-measurement assessors, which could have contributed to interrater error.
The application of kinesiology tape may also have had a high variability in application, as many therapists were involved in its application. Although all therapists applying the tape were trained and received a competency check-off from the study investigators, it is possible that accurate coverage of involved area, pull of tape, and smoothness of tape edges made for comfort could have differed among therapists.
With consideration of intensity of training, there was no specific exercise protocol for all subjects. Consequently, the frequency of exercise was random and based on the normal routine of the treating therapist for each day. Also, patients may have had varying time of 1: 1 treatment with therapy, as they were permitted to participate in group settings. In retrospect, if there was a specified protocol of training with 1: 1 treatments, this may negate the possibility of the intervention group being more conservative with movement due to the application of tape on the involved limb.
Lastly, the small sample size of this study must be considered. Therefore, the ability to show a minimal yet clinically important pretest vs posttest difference was limited. Also, given the use of a single center in addition to the study’s small sample size, the external validity of the study’s results are limited. Future studies are warranted to investigate the effect of kinesiology tape following IM nailing for edema in a larger group of patients. Future studies may be further improved by having a specific training protocol, a smaller number of trained therapists applying tape, and having the same assessor for each subject before and after the intervention.
Conclusions
In this study from a single center, kinesiology tape in patients with intramedullary nailing for femoral shaft fracture did not significantly reduce the volume of the lower limb, reduce pain, or improve postoperative mobility. The only significant improvement from the use of kinesiology tape was improved active knee extension due to improvement in quadriceps force.
References
1. Neumann MV, Südkamp NP, Strohm PC, Management of femoral shaft fractures: Acta Chir Orthop Traumatol Cech, 2015; 82(1); 22-32
2. Paterno M, Archdeacon M, Is there a standard rehabilitation protocol after femoral intramedullary nailing?: J Orthop Trauma, 2009; 23(5 Suppl); S39-46
3. : What is Kinesiotape? Kinesio tape: Made with everyone in mind [Internet], Kinesio University Available from: https://www.kinesiotaping.com/about/what-is-kinesio-tape/
4. Han-Ju T, Hsiu-Chuan H, Jing-Lan Y, Could kinesio tape replace the bandage in decongestive lymphatic therapy for breast-cancer-related lymphedema? A pilot study: Support Care Cancer, 2009; 17(11); 1353-60
5. Sears B, Kinesiology tape in physical therapy [Internet]: Verywell Health [Cited 2020 May 23]. Available from: www.verywell.com/kinesiology-tape-in-physical-therapy-2696435
6. Nijs J, Daenen L, Cras P, Nociception affects motor output: A review on sensory-motor interaction with focus on clinical implications: Clin J Pain, 2012; 28(2); 175-87
7. Mostafavifar M, Wertz J, Borchert J, A systematic review of the effectiveness of kinesio taping for musculoskeletal injury: The Physician and Sports Medicine, 2012; 40; 33-40
8. , Wikipedia.org [Internet]: Hilton’s Law [Cited 2021 Sept 1]. Available from: https://en.wikipedia.org/wiki/Hilton%27s_law
9. Morris D, Jones D, Ryan H, Ryan CJ: Physiother Theory Pract, 2013; 29; 259-70
10. : What is the kinesio taping method? [Internet], Kinesio University Available from: https://www.kinesiotaping.com/about/what-is-the-kinesio-taping-method/
11. , Physiopedia.com [Internet]: Kinesio taping Available from: https://www.physio-pedia.com/Kinesio_Taping
12. Whitaker J, Williams A, Measuring change in limb volume to evaluate lymphoedema treatment outcome: EWMA Journal, 2015; 15
13. Białoszewski D, Woźniak W, Żarek S, Clinical efficacy of kinesiology taping in reducing edema of the lower limbs in patients treated with the Ilizarov method – preliminary report: Ortop Traumatol Rehabil, 2009; 11(1); 46-54
14. Windisch C, Brodt S, Röhner E, Matziolis G, Effects of Kinesio taping compared to arterio-venous Impulse System™ on limb swelling and skin temperature after total knee arthroplasty: Int Orthop, 2017; 41(2); 301-7 [Erratum in: Int Orthop. 2017;41(4):855]
15. Bodian CA, Feedman G, Hossain S, The visual analog scale for pain: Clinical significance in postoperative patients: Anesthesiology, 2001; 95(6); 1356-61
16. Hancock GE, Hepworth T, Wembridge K, Accuracy and reliability of knee goniometry methods: J Exp Orthop, 2018; 5(1); 46
17. , Sralab.org [Internet]: Timed Up and Go Available from: https://www.sralab.org/rehabilitation-measures/timed-and-go
18. Choi IR, Lee JH, Effect of kinesiology tape application direction on quadriceps strength: Medicine (Baltimore), 2018; 97(24); e11038
19. Sharkey AR, King SW, Kuo RY, Measuring limb volume: Accuracy and reliability of tape measurement versus perometer measurement: Lymphatic Research and Biology, 2018; 16; 182-86
In Press
05 Mar 2024 : Clinical Research
Muscular Function Recovery from General Anesthesia in 132 Patients Undergoing Surgery with Acceleromyograph...Med Sci Monit In Press; DOI: 10.12659/MSM.942780
05 Mar 2024 : Clinical Research
Effects of Thermal Insulation on Recovery and Comfort of Patients Undergoing Holmium Laser LithotripsyMed Sci Monit In Press; DOI: 10.12659/MSM.942836
05 Mar 2024 : Clinical Research
Role of Critical Shoulder Angle in Degenerative Type Rotator Cuff Tears: A Turkish Cohort StudyMed Sci Monit In Press; DOI: 10.12659/MSM.943703
06 Mar 2024 : Clinical Research
Comparison of Outcomes between Single-Level and Double-Level Corpectomy in Thoracolumbar Reconstruction: A ...Med Sci Monit In Press; DOI: 10.12659/MSM.943797
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952