28 March 2022: Clinical Research
A Study to Identify the Optimum Forearm Floss Band Intensity in 29 Young Adults Performing Blood Flow Restriction Training
Yongwoo Lee1ABCDEFG*, JaeLim Choi1ABEFDOI: 10.12659/MSM.935771
Med Sci Monit 2022; 28:e935771






Abstract
BACKGROUND: A floss band is used in resistance training and consists of a heavy-duty rubber resistance band to compress a joint or muscle group while performing a range of motion. Blood flow restriction (BFR) training combines low-intensity exercise with occlusion of blood flow, resulting in the effects of high-intensity training. This study aimed to identify the optimum forearm floss band intensity in 29 young adults while performing BFR training.
MATERIAL AND METHODS: Twenty-nine young and healthy adults voluntarily participated in this experiment. One of 4 types of floss bands with different intensities was randomly selected from the subjects and wound around their forearms. The tension of the floss band was calculated to be the length of the participant’s forearm when stretched by 105%, and then wound around the forearm. Blood flow was measured 4 times at regular intervals (pretest: 1 min, during: 2 min, posttest [1]: 1 min, posttest [2]: 2 min) using laser Doppler imaging.
RESULTS: We found that the application of floss bands resulted in a significant interaction between the intensity (colors) and time (pre/during/post) with regard to the hemodynamic changes (P<0.05). The hemodynamic evaluation revealed a reduction in the blood flow (P<0.05).
CONCLUSIONS: This preliminary study shows that the use of blood flow restriction training requires support from guidelines for optimal floss band intensity, particularly with the increasing clinical use of this method.
Keywords: Regional Blood Flow, Compression Bandages, Exercise Therapy, Blood Flow Restriction Therapy, Forearm, Humans, Muscle, Skeletal, resistance training, young adult
Background
Blood flow restriction (BFR) training is a method of training that involves the application of cuffs or bands around the extremities during exercise, in order to maintain the arterial inflow to the muscle while preventing the venous outflow [1]. BFR technique enhances the drainage from blood vessels and lymphatics and prevents the accumulation of tissue fluid in the extravascular space [2]. BFR training combines low-intensity exercise with occlusion of blood flow, resulting in the effects of high-intensity training [3]. Recent research has demonstrated that the effects of muscle-strengthening exercises involving blood flow restriction with loads of 20% of a person’s 1-repetition maximum (RM) is comparable to that of exercises with loads of 60% of 1RM [4]. The benefit of lower loads is reducing mechanical stress on the joints and bones, which is helpful for subjects who have difficulty or contraindicated in lifting near-maximum loads [5].
Mechanical tension that can be attributed to external factors, such as cuffs or bands, can account for the mechanism involved BFR resistance training. When muscle tension is stimulated by external factors, the sarcolemmal-bound mechanosensors, such as integrins and focal adhesions, convert mechanical energy into chemical signals that mediate the intracellular anabolic and catabolic pathways. This results in a shift in the muscle protein balance that induces synthesis over degradation [6].
A previous study by Fujita et al [7] reported that during exercise, muscle fatigue was observed to be accelerated in the stressed areas with BFR. The technique leads to a decrease in oxygen saturation and pH, which results in faster lactate accumulation. Another study, by Takarada et al [8], reported that the release of growth hormone was a consequence of the intramuscular accumulation of lactate. Despite the fact that the low level of mechanical tension associated with BFR resistance training would not significantly affect or induce these mechanisms, metabolic stress has also been shown to mediate similar mechanisms and the effects may be additive [9].
The use of floss bands in sports is becoming popular in countries like Germany and the USA. A floss band is a rubber band made of latex, which is harmless to the human body [10]. The rubber band (2–5 cm in width) is wrapped around a joint or the abdominal muscles, which results in blood flow restriction during training. The floss band has been reported to be a unique entity, compared to the other compressive bands, owing to the fact that it can adhere to the skin without slipping and the users can tighten the band to an optimal level, compared to the other methods. Moreover, the band provides stronger pressure on the tissues during movement, which can result in better myofascial release [11]. In addition, the floss band offers many other advantages, such as improved postintervention ankle range of motion, jump, and sprint performance for up to 45 min in healthy individuals [12,13], reduced pain and improved function in individuals with Achilles tendinopathy [14], reintegrated proprioceptive senses, increased mobility, reduced edema, improved muscle strength, and increased coordination [15].
Despite the fact that floss bands have become popular and have many advantages, there are no standardized recommendations or guidelines regarding the use of floss bands or specifications with regard to the tension to be applied to ensure adequate BFR during resistance training [16]. Furthermore, several recent studies have reported that BFR during resistance training can cause excessive metaboreflex activation and, consequently, an abnormal hemodynamic response during exercise [17–20]. It is recommended to reduce external cuff pressure, pressure application time, and physical exertion when applying BFR to healthy people and especially for people with cardiovascular disease [21].
To improve the insufficient evidenced-based guidelines for applying the floss band, Cheatham et al [16] conducted a kinesiology laboratory-setting experiment with 6 different lengths to quantify the floss band stretch force. However, there is still a lack of evidence for the application of floss bands. Therefore, in this study, we investigated the effect of 4 types of floss bands with different intensities on changes in blood flow in the forearm of healthy adults, as well as assessing the effects of floss bands.
Material and Methods
PARTICIPANTS:
In this study, 29 healthy individuals (18 men, 11 women) were recruited through the mail from among Sahmyook University students. Before the experiment, a sufficient explanation of the purpose, method, and process of the experiment was provided, and an informed consent form was signed, stating that the participant could withdraw from the study at any time if desired. This study was approved by the Research Ethics Committee of Sahmyook University (SYUIRB2018-041). Inclusion criteria were no history of neurological or orthopedic disabilities of the upper extremities, and no learning disabilities or visual impairments [22]. Exclusion criteria were history cardiovascular disease such as deep vein thrombosis and pulmonary embolism, or recently pregnant [23]. The subjects were not permitted to perform strenuous exercises, consume caffeine or alcohol, or smoke within 24 h before commencement of experimental procedures.
PROCEDURE:
The present study involved 29 healthy adults. The researcher provided all the subjects with explanations regarding the experimental procedure until complete comprehension was ensured. Prior to the intervention, the blood flow, blood pressure (measured twice), and circumference and length of the subject’s forearm were measured. Data pertaining to the blood flow were collected by means of 4 trials (4 intensities of floss bands; Lime Green=light, Blueberry=medium, Plum=heavy, Gray=extra heavy) in each subject. The order of application of the floss bands was determined at random by drawing lots. All the floss bands were applied by a single operator (the same researcher).
All the subjects were permitted to enter the laboratory at least 15 min prior to commencement of experimental procedures to ensure a normal and relaxed status. The evaluations were performed in a quiet, temperature-controlled (24°C) room [24]. Floss bands of 4 different intensities were used in this study (COMPRE floss band, 2 m (L)×5 cm (W); Sanctband, Malaysia) (Figure 1). The subjects were comfortably seated on a chair and the testing arm was positioned on a table at the heart level. The floss bands were applied around the bare forearm in a sequence that was chosen at random to reduce bias. The hemodynamic changes were monitored for 6 min (pretest, during, posttest (1), and posttest (2). Owing to the sensitivity of the laser Doppler imaging device, the subjects were strictly prevented from moving or speaking during the evaluations. After each session, the subjects were allowed to sit in a comfortable position and relax for 3 min.
LENGTH AND CIRCUMFERENCE OF THE FOREARM:
The length of the forearm was measured from the tip of the olecranon process to the midpoint of the radial and ulnar tuberosities using a standard measuring tape [25]. The following points were selected to determine the area to apply the floss band to the forearm, and to determine the tension of the floss band, the circumference of the forearm at 4 points was measured. The 4 points were:
To apply the floss band with consistent tension, numbers were marked on the floss band at intervals of 5 mm, like a ruler. Then, using the formula below, the length of the floss band was pulled as far as the length of the forearm and wrapped around the forearm. Each floss band was used for a total of 4 applications. All the floss bands were applied by a single physiotherapist.
Formula:
BLOOD FLOW: The subjects were seated on a chair and the testing arm was positioned on a table at heart level. This study used the right dorsal part of the forearm to achieve a stable position due to the thin layer of subcutaneous fat tissue in the region. A laser target was marked at 1/10 of the length of the forearm, from the center of the distal radial and ulnar tuberosities. Before the intervention, the blood flow to the forearm was evaluated using laser Doppler imaging (LDI) for 1 min. Subsequently, the floss band was wrapped around the forearm. The application of the floss band commenced from the distal to proximal sites to allow better movement. Half of the width of the floss band overlapped during the process of wrapping [16]. During intervention, the blood flow was evaluated by LDI for 2 min. Further evaluations were performed after a period of rest, which entailed the removal of the floss band for 3 min.
LASER DOPPLER IMAGING: WE used a laser Doppler imaging device (moorLDI2-IR, Moor Instrument, Ltd, Millwey, Axminster, Devon, UK) to measure the blood flow, and the sample rate was set at 20 Hz. Areas of the skin that were different in color or included large veins or hematomas were avoided. The LDI device was positioned on separate mounts and fixed perpendicular to the floor, approximately 30 cm above the area of skin to be measured, regardless of the subject’s limb position [26].
A laser beam from the device was directed toward the target. The beam scanned the target, determined by the distance between the device and the target. The laser beam penetrated the skin and the light was dispersed by the mobile red blood cells, which generated a frequency that is detected using a photodetector. The velocity and concentration of the red blood cells generated the shift in Doppler frequency and determined the intensity of the signal. The Doppler shift was expressed in arbitrary perfusion units (PU) [24].
We used moorLDI Single Point Review software version 5.3 for the analysis.
BLOOD PRESSURE:
We used the A&D UA-767 device for the evaluation of blood pressure (UA-767; A&D Company, Ltd, Japan), which is a fully automatic, one-button-operated device.
STATISTICAL ANALYSIS:
The statistical analysis was performed using the SPSS version 21.0 statistical software (IBM, Chicago, IL, USA). The Kolmogorov-Smirnov test was used to confirm the normality of data distribution (
Results
BLOOD FLOW:
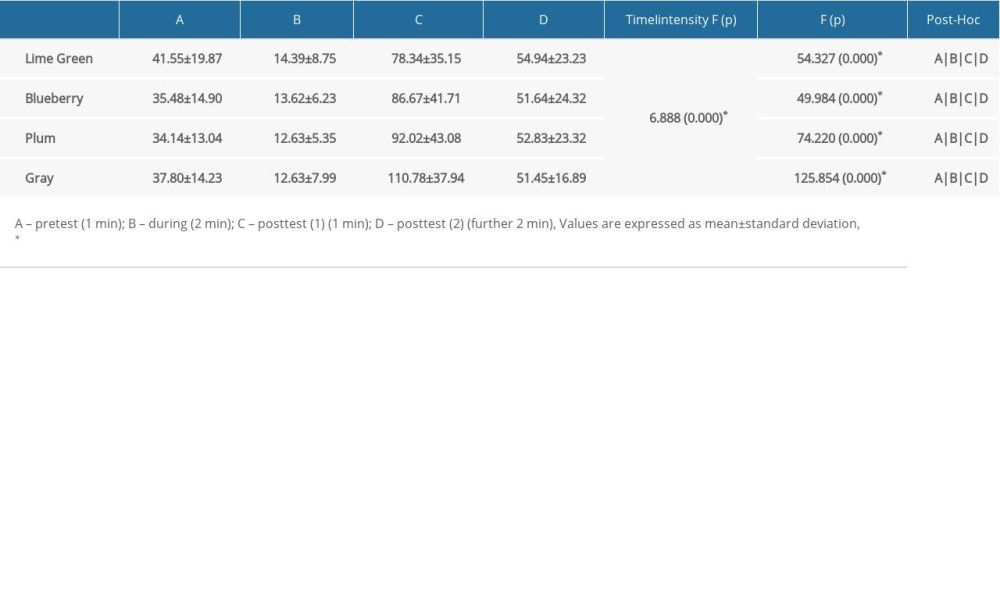
A repeated-measures ANOVA with Greenhouse-Geisser correction revealed that the mean changes pertaining to the blood flow associated with each of the 4 the floss bands differed between the time points and the difference was statistically significant (P<0.05). Moreover, we found statistically significant interactions between the intensity and time (pretest/during/posttest [1]/posttest [2]) with regard to the hemodynamic changes (P<0.05). The results are shown in Table 2 and Figure 2.
Discussion
This study was conducted to supplement the insufficient evidence on applying blood flow restriction training to the forearm using a floss band. In particular, it was carried out to find out how the change of forearm blood flow appears according to the intensity of the floss band. According to the experimental results, the blood flow was significantly decreased during the application compared to before application by the floss bands of 4 different intensities (
Although there are various studies showing clinical effects using floss bands, still lacks evidence-based guidelines [27]. To address this problem, Cheatham et al [16] conducted an experiment to measure the tension along the stretched length using a floss band of 5.08 cm (2 inches) and 10.16 cm (4 inches) using a digital force gauge, showing that the tension increases linearly as the floss band becomes longer. In our study, to apply a constant tension, the length of the floss band extended by 105% was calculated to be the same as the length of the forearm. To extend the same length as the calculated length, we marked the floss band at intervals of 5 mm (like a ruler). Although this method is a limitation of this study, it is also considered to be a method that can be applied in clinical practice in that the length to be stretched is obtained through a certain formula.
Although the current study is the first to evaluate the hemodynamic changes pertaining to the application of floss bands of 4 different intensities (color), the results should be compared to other studies to standardize the implementation of techniques used for blood flow restriction. A study by Mouser et al [28] reported that 2 commonly used cuffs (10-cm and 12-cm) that were inflated to the same pressure on the right thigh generated similar hemodynamic changes. However, Loenneke et al [29] reported that the restrictive cuff pressure should be based on the width of the cuff and stated that circumference is the most significant determinant of the arterial occlusion pressure. Another study, by Rossow et al [30], reported that regardless of the greater physical irritation produced by the wide cuffs (13.5-cm) compared to the narrow (5-cm) cuffs, the use of wide (13.5-cm) cuffs generated a greater elevation in all the cardiovascular and perceptual responses that were evaluated during and after exercises. In addition, limb size and composition have an influence on the pressure levels at which arterial blood flow restriction occurs during the application of cuffs [29]. Recent research on the effects of blood flow restriction involves elastic and non-elastic cuffs of various widths; although several types of bands are in current use, they are usually set at the same standardized pressure during exercise [30]. The aforementioned reasons were the basis for the implementation of the present study. The results of the present study may provide a scientific basis for further research on floss bands.
The exact physiological mechanism associated with the various benefits pertaining to the usage of floss bands has not been fully determined yet. However, previous research that studied other methods of blood flow restriction revealed that the physiological responses were similar. Takano et al [31] reported that low-intensity resistance exercise with blood flow restriction stimulates the release of growth hormone, vascular endothelial growth factor (VEGF), and insulin-like growth factor (IGF), with a decrease in the cardiac preload during exercise. A study by Takarada et al [8] reported that the maximum concentrations of norepinephrine (NE) and lactate (La) were observed immediately after the exercise (0 min) and the maximum concentrations of the growth hormone were observed 15 min after exercise. A study by Wernbom et al [32] reported that blood flow restriction with low-resistance exercise can result in the increased phosphorylation of p70S6K (which has a role in regulating cell motility), which persists for a minimum of 24 h after exercise, and the early phosphorylation of protein kinase p38 (p38MAPK), in addition to the enormous satellite cells in muscle fiber. Thus, it is reasonable to assume that the use of floss bands can provide benefits through the restriction of regional blood flow.
Clinical evaluation of the regional blood perfusion and oxygenation are essential parts of wound management. Oxygen plays an important role in wound healing and the prevention of postoperative infection. The bacteria in the injured area are destroyed by means of the intracellular oxidative mechanisms within the white blood cells, and molecular oxygen is necessary for the production of oxygen radicals, such as bactericidal superoxide [33]. The current study observed a significant elevation in the regional blood flow at 1 min after the application of floss bands. It can be speculated that this could improve wound healing.
This study has certain limitations. First, it had a small sample size. Second, the current study involved only young healthy adults and the results may not apply to the general population that includes individuals of all age groups. Third, the application of floss band was done by the researcher. Finally, despite the fact that the floss band was calibrated, the tension could have varied during the process of wrapping. In view of the fact that only the results pertaining to the application of floss bands on the fore arm were assessed, future research should involve the application of floss bands on other parts of the body, such as the joints or relatively thicker parts.
Conclusions
This preliminary study has highlighted that the use of blood flow restriction training requires support from guidelines for optimal floss band intensity, particularly with the increasing clinical use of this method.
Figures
 Figure 1. Four different intensities of floss bands (COMPRE Floss band, 2 m (L) × 5 cm (W); Sanctband, Malaysia).
Figure 1. Four different intensities of floss bands (COMPRE Floss band, 2 m (L) × 5 cm (W); Sanctband, Malaysia). 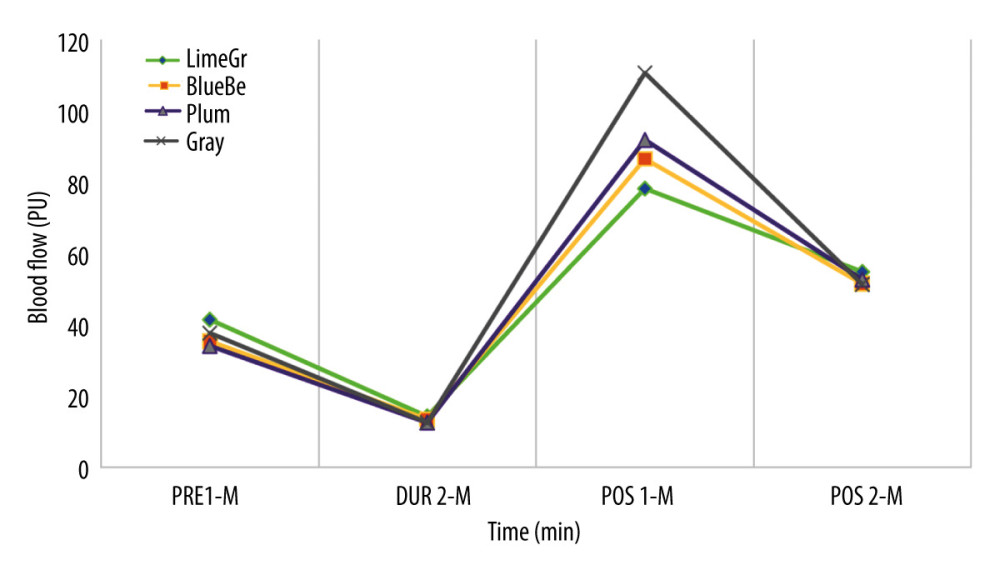 Figure 2. Changes of blood flow by time and floss band intensities (N=29). LimeGr – Lime Green; BlueBe – Blueberry; PRE 1-M – pretest 1-minute,; DUR 2-M – during 2-minutes; POS 1-M – posttest 1-minute; POS 2-M – posttest 2-minutes; PU – perfusion unit.
Figure 2. Changes of blood flow by time and floss band intensities (N=29). LimeGr – Lime Green; BlueBe – Blueberry; PRE 1-M – pretest 1-minute,; DUR 2-M – during 2-minutes; POS 1-M – posttest 1-minute; POS 2-M – posttest 2-minutes; PU – perfusion unit. 
References
1. Ursprung WM: The effects of blood flow restriction training on VO2Max and 1.5 mile run performance, 2016; 29-41, San Antonio, Texas, Texas A&M University-San Antonio
2. Taradaj J, Rosińczuk J, Dymarek R, Comparison of efficacy of the intermittent pneumatic compression with a high-and low-pressure application in reducing the lower limbs phlebolymphedema: Ther Clin Risk Manag, 2015; 11; 1545
3. Bennett H, Slattery F, Effects of blood flow restriction training on aerobic capacity and performance: A systematic review: J Strength Cond Res, 2019; 33; 572-83
4. Loenneke JP, Pujol TJ, The use of occlusion training to produce muscle hypertrophy: Strength & Conditioning Journal, 2009; 31; 77-84
5. Centner C, Wiegel P, Gollhofer A, König D, Effects of blood flow restriction training on muscular strength and hypertrophy in older individuals: A systematic review and meta-analysis: Sports Medicine, 2019; 49; 95-108
6. Zou K, Meador BM, Johnson B, The α7β1-integrin increases muscle hypertrophy following multiple bouts of eccentric exercise: J Appl Physiol, 2011; 111; 1134-41
7. Fujita S, Abe T, Drummond MJ, Blood flow restriction during low-intensity resistance exercise increases S6K1 phosphorylation and muscle protein synthesis: J Appl Physiol, 2007; 103; 903-10
8. Takarada Y, Nakamura Y, Aruga S, Rapid increase in plasma growth hormone after low-intensity resistance exercise with vascular occlusion: J Appl Physiol, 2000; 88; 61-65
9. Pearson SJ, Hussain SR, A review on the mechanisms of blood-flow restriction resistance training-induced muscle hypertrophy: Sports Med, 2015; 45; 187-200
10. Kiefer BN, Lemarr KE, Enriquez CC, A pilot study: Perceptual effects of the voodoo floss band on glenohumeral flexibility: International Journal of Athletic Therapy and Training, 2017; 22; 29-33
11. Kiefer BN, Lemarr KE, Enriquez CC, A pilot study: Perceptual effects of the voodoo floss band on glenohumeral flexibility: Int J Athl Ther Train, 2017; 22; 29-33
12. Driller M, Mackay K, Mills B, Tavares F, Tissue flossing on ankle range of motion, jump and sprint performance: A follow-up study: Physical Therapy in Sport, 2017; 28; 29-33
13. Driller MW, Overmayer RG, The effects of tissue flossing on ankle range of motion and jump performance: Phys Ther Sport, 2017; 25; 20-24
14. Borda J, Selhorst M, The use of compression tack and flossing along with lacrosse ball massage to treat chronic Achilles tendinopathy in an adolescent athlete: A case report: J Man Manip Ther, 2017; 25; 57-61
15. Konrad A, Močnik R, Nakamura M, Effects of tissue flossing on the healthy and impaired musculoskeletal system: A scoping review: Front Physiol, 2021; 12; 577
16. Cheatham SW, Baker R: J Sport Rehabil, 2020; 29; 377-80
17. Domingos E, Polito MD, Blood pressure response between resistance exercise with and without blood flow restriction: A systematic review and meta-analysis: Life Sci, 2018; 209; 122-31
18. Scott BR, Peiffer JJ, Thomas HJ, Hemodynamic responses to low-load blood flow restriction and unrestricted high-load resistance exercise in older women: Front Physiol, 2018; 9; 1324
19. Cristina-Oliveira M, Meireles K, Spranger MD, Clinical safety of blood flow-restricted training? A comprehensive review of altered muscle metaboreflex in cardiovascular disease during ischemic exercise: Am J Physiol Heart Circ Physiol, 2020; 318; H90-109
20. Spranger MD, Krishnan AC, Levy PD, Blood flow restriction training and the exercise pressor reflex: A call for concern: Am J Physiol Heart Circ Physiol, 2015; 309; H1440-52
21. Pope ZK, Willardson JM, Schoenfeld BJ, Exercise and blood flow restriction: J Strength Cond Res, 2013; 27; 2914-26
22. Ahmadi H, Herat N, Alizadeh S, Effect of an inverted seated position with upper arm blood flow restriction on measures of elbow flexors neuromuscular performance: PLoS One, 2021; 16; e0245311
23. Dhokia B, Mabin EO, Bradley WJ, Neal BS, The feasibility, safety, and efficacy of upper limb garment-integrated blood flow restriction training in healthy adults: Pilot Feasibility Stud Feb 8, 2022; 8(1); 34
24. Saez AMO, Mosel F, Nürnberger J, Laser Doppler imager (LDI) scanner and intradermal injection for in vivo pharmacology in human skin microcirculation: Responses to acetylcholine, endothelin 1 and their repeatability: Br J Clin Pharmacol, 2005; 59; 511-19
25. Mohanty BB, Agrawal D, Mishra K, Estimation of height of an individual from forearm length on the population of Eastern India: J Hist Med Allied Sci, 2013; 3; 72
26. Krite Svanberg E, Wollmer P, Andersson-Engels S, Çkeson J, Physiological influence of basic perturbations assessed by non-invasive optical techniques in humans: Appl Physiol Nutr Metab, 2011; 36; 946-57
27. Hodeaux K: The effect of floss bands on elbow range of motion in tennis players, 2017, Fayetteville, AR, University of Arkansas
28. Mouser JG, Dankel SJ, Mattocks KT, Blood flow restriction and cuff width: Effect on blood flow in the legs: Clin Physiol Funct Imaging, 2018; 38; 944-48
29. Loenneke JP, Fahs CA, Rossow LM, Effects of cuff width on arterial occlusion: Implications for blood flow restricted exercise: Eur J Appl Physiol, 2012; 112; 2903-12
30. Rossow LM, Fahs CA, Loenneke JP, Cardiovascular and perceptual responses to blood flow restricted resistance exercise with differing restrictive cuffs: Clin Physiol Funct Imaging, 2012; 32; 331-37
31. Takano H, Morita T, Iida H, Hemodynamic and hormonal responses to a short-term low-intensity resistance exercise with the reduction of muscle blood flow: Eur J Appl Physiol, 2005; 95; 65-73
32. Wernbom M, Apro W, Paulsen G, Acute low-load resistance exercise with and without blood flow restriction increased protein signalling and number of satellite cells in human skeletal muscle: Eur J Appl Physiol, 2013; 113; 2953-65
33. Gottrup F, Oxygen in wound healing and infection: World J Surg, 2004; 28; 312-15
Figures
Figure 1. Four different intensities of floss bands (COMPRE Floss band, 2 m (L) × 5 cm (W); Sanctband, Malaysia).Figure 2. Changes of blood flow by time and floss band intensities (N=29). LimeGr – Lime Green; BlueBe – Blueberry; PRE 1-M – pretest 1-minute,; DUR 2-M – during 2-minutes; POS 1-M – posttest 1-minute; POS 2-M – posttest 2-minutes; PU – perfusion unit. In Press
05 Mar 2024 : Clinical Research
Role of Critical Shoulder Angle in Degenerative Type Rotator Cuff Tears: A Turkish Cohort StudyMed Sci Monit In Press; DOI: 10.12659/MSM.943703
06 Mar 2024 : Clinical Research
Comparison of Outcomes between Single-Level and Double-Level Corpectomy in Thoracolumbar Reconstruction: A ...Med Sci Monit In Press; DOI: 10.12659/MSM.943797
21 Mar 2024 : Meta-Analysis
Economic Evaluation of COVID-19 Screening Tests and Surveillance Strategies in Low-Income, Middle-Income, a...Med Sci Monit In Press; DOI: 10.12659/MSM.943863
10 Apr 2024 : Clinical Research
Predicting Acute Cardiovascular Complications in COVID-19: Insights from a Specialized Cardiac Referral Dep...Med Sci Monit In Press; DOI: 10.12659/MSM.942612
Most Viewed Current Articles
17 Jan 2024 : Review article
Vaccination Guidelines for Pregnant Women: Addressing COVID-19 and the Omicron VariantDOI :10.12659/MSM.942799
Med Sci Monit 2024; 30:e942799
14 Dec 2022 : Clinical Research
Prevalence and Variability of Allergen-Specific Immunoglobulin E in Patients with Elevated Tryptase LevelsDOI :10.12659/MSM.937990
Med Sci Monit 2022; 28:e937990
16 May 2023 : Clinical Research
Electrophysiological Testing for an Auditory Processing Disorder and Reading Performance in 54 School Stude...DOI :10.12659/MSM.940387
Med Sci Monit 2023; 29:e940387
01 Jan 2022 : Editorial
Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-Hospitalized Pa...DOI :10.12659/MSM.935952
Med Sci Monit 2022; 28:e935952